 DE
DE FR
FR IT
IT ES
ES



Lasix
Active substance — Furosemide
Pharmachologic effect
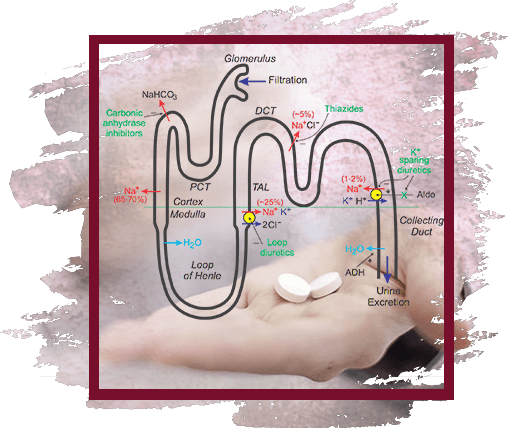
"Loop" diuretic. Violates the reabsorption of sodium and chlorine ions in the thick segment of the ascending part of Henle's loop. Due to the increase in the release of sodium ions, there is a secondary (mediated by osmotically bound water) enhanced excretion of water and an increase in the secretion of potassium ions in the distal part of the renal tubule. At the same time, the excretion of calcium and magnesium ions increases.
Has secondary effects due to the release of intrarenal mediators and the redistribution of intrarenal blood flow. Against the background of the course of treatment, there is no weakening of the effect.
In heart failure, it quickly leads to a decrease in the preload on the heart through the expansion of large veins. It has a hypotensive effect due to an increase in the excretion of sodium chloride and a decrease in the reaction of vascular smooth muscles to vasoconstrictor effects and as a result of a decrease in the BCC. The effect of furosemide after intravenous administration occurs within 5-10 minutes; after oral administration - after 30-60 minutes, maximum action - after 1-2 hours, duration of effect - 2-3 hours (with reduced renal function - up to 8 hours). During the period of action, the excretion of sodium ions increases significantly, but after its termination, the rate of excretion decreases below the initial level ("rebound" or "cancellation" syndrome). The phenomenon is caused by a sharp activation of the renin-angiotensin and other antinatriuretic neurohumoral regulation links in response to massive diuresis; stimulates the arginine-vasopressive and sympathetic systems. Reduces the level of atrial natriuretic factor in plasma, causes vasoconstriction.
Due to the phenomenon of "rebound" when taken 1 time / day may not have a significant effect on the daily excretion of sodium ions and blood pressure. When administered intravenously, it causes dilatation of peripheral veins, reduces preload, reduces left ventricular filling pressure and pulmonary artery pressure, as well as systemic blood pressure.
The diuretic effect develops 3-4 minutes after intravenous administration and lasts 1-2 hours; after oral administration - after 20-30 minutes, lasts up to 4 hours.
Pharmacokinetics
After oral administration, absorption is 60-70%. In severe kidney disease or chronic heart failure, absorption decreases.
Vd is 0.1 l / kg. Plasma protein binding (mainly albumin) - 95-99%. Metabolized in the liver. It is excreted by the kidneys - 88%, with bile - 12%. T1 / 2 in patients with normal kidney and liver function is 0.5-1.5 hours. With anuria, T1 / 2 can increase to 1.5-2.5 hours, with combined renal and hepatic insufficiency - up to 11-20 hours.
Indications
Edema syndrome of various origins, incl. with chronic heart failure stage II-III, liver cirrhosis (portal hypertension syndrome), nephrotic syndrome. Pulmonary edema, cardiac asthma, cerebral edema, eclampsia, forced diuresis, severe arterial hypertension, some forms of hypertensive crisis, hypercalcemia.
Dosage regimen
Set individually, depending on the indications, clinical situation, age of the patient. During treatment, the dosage regimen is adjusted depending on the magnitude of the diuretic response and the dynamics of the patient's condition.
For oral administration, the initial dose for adults is 20-80 mg / day, then, if necessary, the dose is gradually increased to 600 mg / day. For children, a single dose is 1-2 mg / kg.
The maximum oral dose for children is 6 mg / kg.
With intravenous (jet) or intramuscular administration, the dose for adults is 20-40 mg 1 time / day, in some cases - 2 times / day. For children, the initial daily dose for parenteral administration is 1 mg / kg.
Side effect
- From the side of the cardiovascular system: lowering blood pressure, orthostatic hypotension, collapse, tachycardia, arrhythmias, decreased BCC.
- From the side of the central nervous system and peripheral nervous system: dizziness, headache, myasthenia gravis, calf muscle cramps (tetany), paresthesia, apathy, weakness, weakness, lethargy, drowsiness, confusion.
- From the senses: impaired vision and hearing.
- From the digestive system: decreased appetite, dry mouth, thirst, nausea, vomiting, constipation or diarrhea, cholestatic jaundice, pancreatitis (exacerbation).
- From the genitourinary system: oliguria, acute urinary retention (in patients with prostatic hypertrophy), interstitial nephritis, hematuria, decreased potency.
- From the hematopoietic system: leukopenia, thrombocytopenia, agranulocytosis, aplastic anemia.
- From the side of water and electrolyte metabolism: hypovolemia, dehydration (risk of thrombosis and thromboembolism), hypokalemia, hyponatremia, hypochloremia, hypocalcemia, hypomagnesemia, metabolic alkalosis.
- Metabolic disorders: hypovolemia, hypokalemia, hyponatremia, hypochloremia, hypokalemic metabolic alkalosis (as a result of these disorders - arterial hypotension, dizziness, dry mouth, thirst, arrhythmia, muscle weakness, convulsions), hyperuricemia (with possible exacerbation of gout)
- Allergic reactions: purpura, urticaria, exfoliative dermatitis, exudative erythema multiforme, vasculitis, necrotizing angiitis, pruritus, chills, fever, photosensitivity, anaphylactic shock.
- Others: with intravenous administration (optional) - thrombophlebitis, renal calcification in premature babies.
Contraindications
Acute glomerulonephritis, stenosis of the urethra, obstruction of the urinary tract with a stone, acute renal failure with anuria, hypokalemia, alkalosis, precomatous conditions, severe hepatic failure, hepatic coma and precoma, diabetic coma, hyperglycemic coma, stenagral, or aorticosteroids hypertrophic obstructive cardiomyopathy, increased central venous pressure (more than 10 mm Hg), arterial hypotension, acute myocardial infarction, pancreatitis, impaired water and electrolyte metabolism (hypovolemia, hyponatremia, hypokalemia, hypochloremia, hypocalcemia, hypomagnesemia, intoxication), intoxication sensitivity to furosemide.
Application during pregnancy and lactation
During pregnancy, the use of furosemide is possible only for a short time and only if the intended benefit of therapy to the mother outweighs the potential risk to the fetus.
Since furosemide can be excreted in breast milk, as well as suppress lactation, if necessary, use during lactation, breastfeeding should be discontinued.
Special instructions
Use with caution in prostatic hyperplasia, SLE, hypoproteinemia (risk of ototoxicity), diabetes mellitus (decreased glucose tolerance), with stenosing atherosclerosis of the cerebral arteries, against the background of prolonged therapy with cardiac glycosides, in elderly patients with severe atherosclerosis (especially pregnancy first half), lactation period.
Before starting treatment, electrolyte disturbances should be compensated for. During the period of treatment with furosemide, it is necessary to control blood pressure, the level of electrolytes and glucose in the blood serum, liver and kidney function.
For the prevention of hypokalemia, it is advisable to combine furosemide with potassium-sparing diuretics. With the simultaneous use of furosemide and hypoglycemic drugs, a dose adjustment of the latter may be required.
It is not recommended to mix the furosemide solution in the same syringe with any other drugs.
Influence on the ability to drive vehicles and use mechanisms
When using furosemide, the likelihood of a decrease in the ability to concentrate cannot be ruled out, which is important for people driving vehicles and working with mechanisms.
Drug interactions
With simultaneous use with antibiotics of the aminoglycoside group (including with gentamicin, tobramycin), an increase in nephro- and ototoxic action is possible.
Furosemide reduces the clearance of gentamicin and increases plasma concentrations of gentamicin, as well as tobramycin.
With simultaneous use with antibiotics of the cephalosporin group, which can cause renal dysfunction, there is a risk of increased nephrotoxicity.
With simultaneous use with beta-adrenergic agonists (including fenoterol, terbutaline, salbutamol) and with corticosteroids, hypokalemia may increase.
With simultaneous use with hypoglycemic agents, insulin, it is possible to reduce the effectiveness of hypoglycemic agents and insulin, because furosemide has the ability to increase plasma glucose.
With simultaneous use with ACE inhibitors, the antihypertensive effect is enhanced. Severe arterial hypotension is possible, especially after taking the first dose of furosemide, apparently due to hypovolemia, which leads to a transient increase in the hypotensive effect of ACE inhibitors. The risk of impaired renal function increases and the development of hypokalemia is not excluded.
With simultaneous use with furosemide, the effects of non-depolarizing muscle relaxants are enhanced.
With simultaneous use with indomethacin, other NSAIDs, a decrease in the diuretic effect is possible, apparently due to inhibition of the synthesis of prostaglandins in the kidneys and sodium retention in the body under the influence of indomethacin, which is a nonspecific COX inhibitor; decrease in antihypertensive action.
It is believed that furosemide interacts in a similar way with other NSAIDs.
When used simultaneously with NSAIDs, which are selective inhibitors of COX-2, this interaction is expressed to a much lesser extent or practically absent.
With simultaneous use with astemizole, the risk of developing arrhythmias increases.
With simultaneous use with vancomycin, an increase in oto- and nephrotoxicity is possible.
With simultaneous use with digoxin, digitoxin, an increase in the toxicity of cardiac glycosides is possible, associated with the risk of hypokalemia while taking furosemide.
There are reports of the development of hyponatremia with simultaneous use with carbamazepine.
With simultaneous use with cholestyramine, colestipol, absorption and diuretic effect of furosemide decreases.
With simultaneous use with lithium carbonate, it is possible to enhance the effects of lithium due to an increase in its concentration in blood plasma.
With simultaneous use with probenecid, the renal clearance of furosemide decreases.
With simultaneous use with sotalol hypokalemia and the development of ventricular arrhythmias of the "pirouette" type are possible.
With simultaneous use with theophylline, it is possible to change the concentration of theophylline in blood plasma.
With simultaneous use with phenytoin, the diuretic effect of furosemide is significantly reduced.
After intravenous administration of furosemide against the background of chloral hydrate therapy, an increase in sweating, a feeling of fever, instability of blood pressure, tachycardia is possible.
With simultaneous use with cisapride, hypokalemia may increase.
It is assumed that furosemide can reduce the nephrotoxic effect of cyclosporine.
With simultaneous use with cisplatin, an increase in the ototoxic effect is possible.





